Date: October 4, 2025
Marc Gosselin MD
Theme: Pediatrics, austere environments and health equity: better understanding physiology for better intervention.
Introduction
The second day of CAWM 2025 was an impressively rich one, with a succession of clinical presentations, field experiences and reflections on the practice of medicine in isolated environments.
Once again, a lot of content to digest - in small bites!
Among my favorites:
- Matthew Smith's masterful review of the pediatric triad (appearance, respiration, circulation), with a practical reminder: sternal capillary return is more reliable than peripheral in newborns and infants - a simple detail, but critical in the field.
- Dr. David Jerome's presentation on tourniquet management in austere settings: clear, practical, and directly applicable to advanced first aid. Removing a tourniquet after 2 to 6 hours - or worse, after 6 hours - involves major metabolic risks and should be reserved for trained professionals. In the event of danger, first apply "High and Tight", then convert as soon as the situation allows.
- A clinical pearl: the demonstration of cooling via the palms, soles and cheeks, three "super-thermal highways" capable of evacuating up to 50% of the efficiency of full immersion! An essential alternative when immersion is impossible or during transport - and confirmation that the old "armpit, groin and neck" methods are a thing of the past.
- Finally, a shocking reminder: carbon monoxide at high altitude still kills. Recent deaths on Mount Rainier are a reminder that symptoms can mimic high-altitude cerebral edema (OCHA). When in doubt, treat for both - 100% oxygen and dexamethasone - without waiting for diagnostic certainty.
And of course, many other fascinating presentations on pediatrics, cold physiology, health equity and leadership in extreme conditions.
A busy, stimulating day, and a constant source of inspiration for those who practice first aid and wilderness medicine
1. Opening presentation
Confiance et leadership à hautes conséquences - Christian Spenner
Background and speaker profile
Christian Stenner is one of Canada's most experienced explorers of glaciovolcanic caves, the cavities formed at the meeting of fire and ice, where gases and steam sculpt glaciers over active volcanoes.
Co-founder of the Bisaro Caves Project, recognized as Expedition of the Year by the Royal Canadian Geographical Society, he helped confirm Bisaro Anima as the deepest cave in the country.
A Fellow of the Royal Canadian Geographical Society, the Explorers Club and National Geographic Explorer, he combines over 25 years' experience in corporate security and crisis management with training in organizational resilience (MSc).
Presentation objectives
- Illustrate how citizen science and individual passion can generate unprecedented scientific breakthroughs, such as the first direct measurements of a Canadian volcano.
- Demonstrate that mutual trust, clarity of intent and informed delegation are the foundations of leadership in high-risk environments.
- Transpose these lessons to medicine in remote areas, where team performance is based on similar values: autonomy, communication and collective commitment.
Key messages and learning
- The "Mission Command" model (clear intent, decentralized execution) provides a structure that allows each team member to act autonomously without losing sight of the overall mission.
- "The best decisions are often made by those closest to the danger." - C. Stenner
- Trust precedes competence in the perception of a team: social psychology research (Amy Cuddy, Susan Fiske) confirms that perceived warmth and reliability first establish a leader's credibility.
- "Confidence is the currency of performance in extreme situations."
- Effective leadership relies on the ability to "embrace honest mistakes": tolerating and learning from failed initiatives, rather than punishing reasoned risk-taking.
- Risk management is based on shared understanding: identifying areas of uncertainty, reducing exposure and anticipating consequences.
- Exploration and isolated medicine environments share a common requirement: to act quickly, decide together, and accept risk without sacrificing safety.
2. Pediatric assessment in isolated settings
Pediatric Assessment in a Wilderness Context — Matthew
Smith
Presenter: Matthew Smith - Critical Care Flight Paramedic, BCEHS; prehospital medicine educator and founder of Canadian Outdoor Med
Context
Matthew Smith, a flight critical care paramedic with British Columbia Emergency Health Services (BCEHS), has dedicated his career to training responders to operate effectively in the most demanding environments - from Vancouver hospitals to British Columbia's rugged terrain.
His presentation on pre-hospital pediatric emergencies offered a no-nonsense, pragmatic approach, suited to austere settings where equipment, personnel and medical support are limited.
Challenges and field perspective
Pediatric emergencies, rare but dreaded, represent a particular challenge for isolated teams.
Matthew Smith highlighted the discrepancies between hospital theory and pre-hospital reality, reminding us that most errors occur not through lack of knowledge, but through stress, improvisation or lack of child-friendly cues.
"The child is not a small adult - he's a patient who compensates differently, communicates differently, and breaks down faster." - Matthew Smith
In remote areas, where access to a doctor or air transport is delayed, this detailed understanding becomes vital. Workers must know how to assess visually, prevent hypothermia, and stabilize before moving.
Rapid recognition model: the paediatric triad
Smith introduced the Pediatric Emergency Assessment Triad, a simple but frighteningly effective tool for early detection of vital distress:
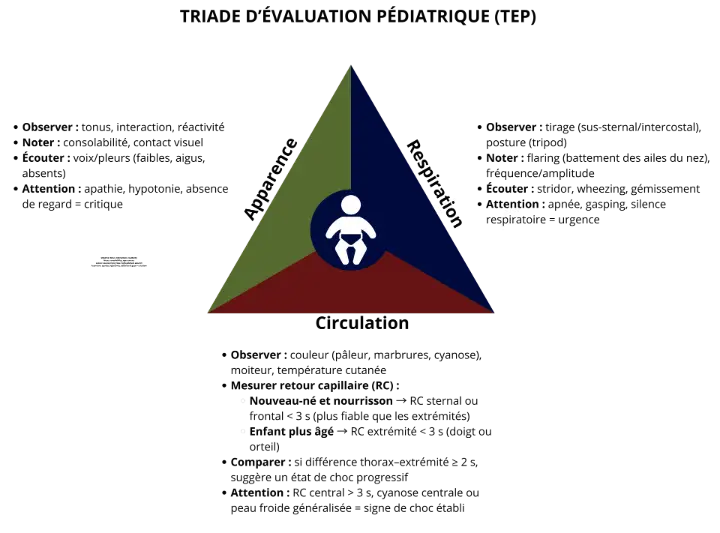
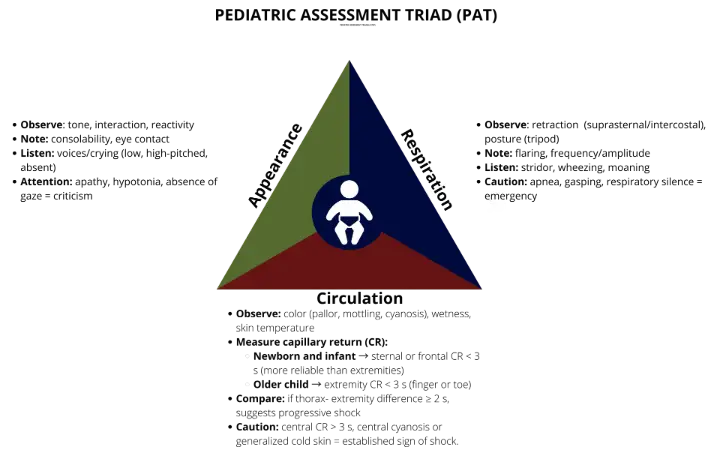
The Pediatric Assessment Triangle (PAT) is a rapid assessment tool that makes it possible to estimate the severity of a child's condition in seconds, even before touching him or her.
It is based on three simple but highly revealing observations:
- Appearance - tone, interactivity and consolability are assessed, reflecting the child's neurological and metabolic state.
- Respiratory work - we observe effort, position, respiratory sounds (stridor, grunting) and frequency, essential for recognizing ventilatory distress.
- Circulation to the skin - we examine skin coloration and especially the sternal capillary return, which is more reliable than the peripheral return in infants and young children.
An abnormality in just one of these components already indicates distress; combined abnormalities often signal rapid cardio-respiratory decompensation.
"In the mountains, in a tent or a remote outpost, you won't always have a monitor - but you'll always have your eyes."
This visual, reproducible and rapid approach can be easily integrated into advanced first aid training in remote areas (WAFA, WFR), and enables non-medical responders to prioritize life-saving procedures efficiently.
Key messages for medicine in remote areas
- Prepare before intervening. Anticipate pediatric emergencies with appropriate protocols and calibrated kits (masks, cuffs, low-volume syringes). A simple Broselow tape can save precious seconds.
- Preserving heat and energy. Children lose heat four times faster than adults. In alpine conditions, a hypothermic patient rapidly becomes bradycardic, compounding diagnostic confusion.
- Breathe first, measure later. The majority of pediatric emergencies are respiratory: obstruction, asthma, drowning, anaphylaxis. Smith stressed the importance of ventilating early, gently and effectively, before thinking about numbers.
- Supporting caregivers and the team. Parent or team stress can amplify the risk of error. Smith encourages verbalizing observations and using simple language: "I see he's breathing fast - let's continue the oxygen."
- Teach clarity, not complexity. The best remote training programs rely on mnemonic tools, realistic simulations and conscious repetition, rather than hospital algorithms that are difficult to apply in the field.
Educational scope
Matthew Smith, Director of Canadian Outdoor Med, advocates a rethink of advanced first aid in austere environments, focusing on practical skills, critical thinking and communication.
His teaching is in line with the CAWM philosophy: train to understand, not to recite.
"The best emergency kit is your calm. Everything else is just incidental." - Matthew Smith
Conclusion
At a conference where science rubs shoulders with field experience, Matthew Smith reminded us that the survival of a child in an isolated environment depends less on technology than on preparation, observation and shared trust within the team.
3. Management of severe bleeding and use of tourniquets
Management of Life-Threatening Bleeding and Tourniquet Use — Dr Dave Jerome
Context
Dr. David Jerome, emergency physician and member of the Canadian Armed Forces, presented a dense and powerful lecture on the rational use of tourniquets in the management of severe hemorrhage.
His experience, both military and civilian, gives him a clear vision: the tourniquet is a survival tool when used correctly - but also a potential risk if poorly taught or applied indiscriminately.
This presentation resonated particularly with participants involved in first aid in remote areas, where the line between pre-hospital care and extended emergency medicine often blurs.
"The tourniquet is not a failure to treat a bleed: it is a decisive clinical decision." - Dr Jerome
Challenges and general framework
- Whether in a military context or a wilderness environment, tourniquets have saved thousands of lives.
- The issue is no longer whether to install one, but when and how to remove it safely - especially when evacuation is delayed.
- Critical time windows of ischemia tolerance (0-2 h, 2-6 h, 6+ h) guide strategy and directly influence limb survival.
- Controlled conversion of the tourniquet - rather than its outright removal - becomes the key step in re-evaluation.
Key messages for the field
- A properly applied tourniquet saves lives. Military and civilian data confirm a reduction in mortality of over 60% when the tourniquet is applied quickly at the point of injury.
-
Removing the tourniquet is a planned medical procedure, not a reflex gesture.
- Always plan a controlled withdrawal, never "cycle" a tourniquet in the field. (The ancient practice of releasing it periodically to "let the blood flow" is formally contraindicated: it restarts hemorrhaging and promotes shock and acidosis).
- Removal can only be carried out in a safe environment, with bleeding monitored and the ability to apply a tourniquet immediately.
-
Differentiate decision zones according to the duration of application:
- 0-2 h (green zone): low risk of reperfusion syndrome; conversion possible as soon as conditions permit.
- 2-6 h (yellow zone): limb salvage window, but high risk of metabolic disorder; release only if all means of management are ready.
- 6+ h (red zone): extreme risk of reperfusion; do not remove tourniquet until you are in a center capable of managing systemic complications.
Extended withdrawal sequence: the ABCD of reperfusion
Inspired by the Australian military approach, this sequence illustrates the preparatory measures to be taken prior to the removal of a prolonged tourniquet, depending on the risks associated with this gesture, hence the importance of proceeding rapidly if a conversion is being considered during tourniquet placement.
Although it is mainly hospital-based, it is still useful for instructors and staff working in isolated environments to know, in order to anticipate pathophysiology and management during transfer.
| Letter | Element | Clinical Objective | Exmple of intervention |
|---|---|---|---|
| A – Alkalosis | Administer sodium bicarbonate | Correct anticipated metabolic acidosis | 1 ampoule of bicarbonate IV before withdrawal |
| B – Blood pressure | Ensure adequate blood volume | Preventing post-reperfusion hypotension | Keep PAM stable before release |
| C – Calcium | Protecting the myocardium | Avoid hyperkalemia and rhythm disorders | 1 g calcium gluconate or chloride IV |
| D – Defibrillation | Monitor heart rate | Anticipating severe arrhythmias | ECG monitoring or pads ready when needed |
"Reperfusion is not relief, it's metabolic stress. Treat it as a critical event." - Dr. Jerome
In isolated environments, the practical application can be summed up as follows: stabilize the patient, prevent hypothermia, document exposure time, and prepare for continuity of care (remote medical assistance, priority transport to an equipped center).
Outlook for rescue services in remote areas
Dr. Jerome pointed out that tourniquet management is now a basic skill in advanced first aid, but that the quality of teaching remains uneven.
He pleads for :
- Standardized teaching, including recognition of situations justifying immediate application ("care under fire") and those where conversion is possible.
- Practical demonstrations based on real-life cases of prolonged extrication, common in industrial regions or remote expeditions.
- The integration of temporality (2 h / 6 h) in advanced first aid training modules.
- A "decision-making" pedagogy: learning to evaluate, not just to apply.
"To teach the tourniquet without teaching when to remove it is to deliver only half the message." - Dr. Jerome
Pedagogical application
For wilderness medicine trainers and instructors :
- Introduce the notion of controlled conversion in simulations.
- Teach progressive bleeding control: release slowly over 60 seconds while observing the wound.
Conclusion
Dr. Jerome's lecture reminded us that tourniquet use is much more than a technical gesture: it's a strategic choice between life, limb and metabolic risk.
In the context of first aid training in remote areas, his message highlights the need to teach not just action, but clinical reflection - the kind that saves a life without compromising another.
"The courage to act must always be accompanied by the courage to wait." - Dr David Jerome
4. Student presentations - Promoting the next generation of doctors in remote areas
This series of mini-conferences highlighted the new generation of clinicians and researchers with a passion for medicine in isolated environments. Under the guidance of experienced mentors, these students presented applied research projects rooted in the realities of the field: pre-hospital care, prevention, leadership, and clinical adaptation in environments where every decision counts.
"Their curiosity, rigor and grounding in the reality of isolated regions are a reminder that innovation in wild medicine is often born in the field, long before it is formalized as science."
4.1. Carbon monoxide poisoning in nature medicine: Risks associated with stoves, tents and snow shelters
Présentée par : Ainsley Johnstone
At high altitudes, carbon monoxide (CO) poisoning can mimic acute mountain sickness, making diagnosis particularly tricky.
Ainsley Johnstone pointed out that symptoms such as headache, fatigue and nausea, often attributed to altitude hypoxia, can mask hypoxia of toxic origin.
- Key physiology: CO binds to hemoglobin with around 200 times greater affinity than oxygen, reducing O₂ availability and shifting the dissociation curve to the left. En altitude, la pression partielle d’oxygène déjà abaissée amplifie ce phénomène : une concentration “modérée” de CO peut produire une hypoxie sévère.
- Risk factors: use of stoves or lanterns in poorly ventilated shelters, cumulative exposure during long expeditions, poorly adjusted vehicles.
- Prevention: minimum ventilation of 50 cm², watch for flames (blue = complete combustion), use tents rather than snow shelters.
- Management: high-flow oxygen as soon as suspected; COHb half-life increases from 6 h (room air) to 80 min under O₂.
In remote areas, empirical treatment for both diagnoses (AMS + CO) can save a life when access to formal diagnosis is impossible.
4.2. Determining Patient Reliability in Spinal Cord Protection: Challenges in the Ski Patrol Setting
Présentée par : Sean Harrop
Ski patroller turned medical student Sean Harrop explored the discrepancy between urban spinal protection protocols and the reality of an isolated alpine environment.
- Observation: Rules such as NEXUS or the Canadian C-Spine Rule are difficult to apply on the slopes: noise, cold, stress, bulky equipment.
- Observation: Patrollers often replace the Glasgow Coma Scale (GCS) with an Alert & Oriented (A&O) test, which increases the number of "if in doubt, immobilize" patients.
- Risk: Over-immobilization can be harmful: discomfort, hypothermia, and risk of increased intracranial pressure.
-
Areas for improvement :
- Simplify GCS criteria for the field (e.g. focus on the motor component).
- Introduce post-extraction reassessment (if A&O = GCS 15, conservative release).
- Train patrollers in distraction recognition and clinical communication.
In remote stations without a medical team, an approach based on "patient reliability" and sound clinical judgment can reduce unnecessary transport while preserving safety.
4.3. Breaking Trails: Women in Wilderness Medicine and the Art of Adventuring Beyond Limits
Présentée par : Kacylia Roy Proulx
This inspiring presentation addressed the place of women in wilderness medicine and the persistent obstacles: under-representation, cultural and logistical biases, and lack of role models.
- Key data: Women make up around 28% of WMS members, but only 22% of published authors.
- Challenges: Unsuitable equipment, lack of privacy in the field, increased mental workload due to social expectations.
-
Call to action:
- Promote gender diversity in expedition teams: diversity = resilience.
- Train leaders to spot bias and build inclusive environments.
- Promoting women in panels, publications and positions of responsibility.
Wild medicine needs the same diversity as the ecosystems it protects.
4.4. Cheeks, Palms, and Soles: Cooling Superhighways for Managing Heat Illness
Présentée par : Connor Haas
Based on the Wilderness Medical Society's 2024 guidelines, this presentation revisited the physiology of thermoregulation and effective cooling methods in the field.
- Principle: Hairless areas (cheeks, palms, soles) have arteriovenous anastomoses (AVAs) that enable rapid heat dissipation.
- Efficiency: Glabrous skin cooling can reach 0.08-0.12°C/min, about half the cooling rate achieved by full immersion (0.15-0.20°C/min), but far superior to traditional methods (armpit/groin).
-
Recommandation :
- Avoid classic sites (armpits, neck, groin): limited effectiveness, risk of discomfort.
- In the absence of cold-water immersion, prioritize cooling of AVA-rich, easily accessible, well-perfused areas (cheeks, palms and soles).
- Stop cooling when neurological signs improve or rectal temperature approaches 38.9°C.
In the field, aim for simplicity: three cold spots, a calm team, and continuous surveillance.
4.5. Little Explorers, Big Challenges: Balancing Risk and Safety in Pediatric Wilderness Medicine
Presented by : Constance de Schaetzen
Constance de Schaetzen has proposed an innovative framework for integrating "Smart Risk" in the pediatric context.
The aim: to strengthen children's resilience and competence without doing away with adventure.
-
Highlights :
- Injuries to children under 15 account for nearly a quarter of all outdoor incidents.
- The average age of those injured was 10; only 7.5% were wearing helmets.
-
Tools proposed :
- Consequence scale: death = change of plan; hospitalization = tightening of controls; bruises = learning zone.
- Three prevention levers (from the NOLS model): preparation, planning, anticipation.
- Active coaching: replace "be careful" with questions ("do you feel stable?", "what could change?").
- Regional challenges: Adapting prevention programs to Canada's mountainous and northern environments, where access to specialized pediatric care is limited.
In wilderness medicine, protecting children is not about eliminating risk; it's about learning to navigate it.
4.6. Identification and Management of Post-Traumatic Hypothermia in the Pre-Hospital Environment
Presented by : Taylor Krawec
Taylor Krawec reminded us that the prevention of traumatic hypothermia is often neglected, even though it is part of the lethal triad (hypothermia, coagulopathy, acidosis).
- Even a temperature of 36°C can worsen the prognosis.
- Field approach: combine passive insulation (layers, vapor barrier) and active heat (chemical compresses on chest and groin).
- Key tool: the "thermal burrito", a multifunctional layer that reduces heat loss through conduction, convection, radiation and evaporation.
- Message for first-aiders: Hypothermia is a systemic problem, not a material one: the key lies in training, planning and rigorous teamwork.
4.7. Exploring Wilderness Medicine in the Care of Remote Communities in Canada
Presented by : Adrienne Teske
Adrienne Teske concluded the session with a societal theme: equitable access to healthcare in remote communities.
Based on a narrative review of 29 articles, she illustrated how medicine in austere environments can build local capacity and act as a bridge to community health.
-
Areas for consideration :
- Train community members in basic emergency response.
- Deploy tele-expertise to guide critical decisions from a distance.
- Aligning wilderness medicine with the principles of equity and aboriginal autonomy.
Remote medicine is not a temporary solution: it's a healthcare architecture based on local resilience.
Conclusion – Jour 2 : relier la science, le terrain et la communauté
The second day of CAWM 2025 vividly illustrated that medicine in austere environments relies on a balance of scientific rigor, pragmatic adaptation and trust in local teams and communities.
Whether it's saving a child in respiratory distress, managing a tourniquet that's been applied for hours, preventing traumatic hypothermia or teaching intelligent risk to a new generation of explorers, the common thread remains the same: preparing humans and systems to function when all is uncertain.
Cross-disciplinary themes
- Physiology guides the decision. Understanding the body - whether hypoxic, hypothermic or pediatric - remains the basis of good clinical decision-making, especially without supporting technology.
- Adapt the protocol without betraying the principle. In isolation, flexibility is a sign of competence: respect the intention of the protocol, even when the means differ.
- Training systems, not just individuals. Survival does not depend solely on the most competent caregiver, but on the link between training, equipment, communication and logistics.
- Building local capacity for sustainable equity. Medicine in isolated regions cannot be parachuted in: it must take root in communities through training, tele-expertise and autonomy.
Key messages
- Act early: oxygen before certainty, warmth before shivering, tourniquets before exsanguination. In the face of uncertainty, inaction is more costly than thoughtful action.
- Children have a unique physiology: adapting rhythm, hydration and thermoregulation. Pediatric medicine in an isolated environment demands anticipation and clinical benevolence.
- Distributed, confident leadership saves time and lives. The best teams share meaning, not just orders.
- Equity requires shared competence and community empowerment. Transmitting knowledge means extending the scope of care beyond the caregiver: it means building collective resilience.
Bonus: Day 3 - Opening conference
“Risk-Managed Mountain Rescue” — Mike Koppang
Kananaskis Resident Specialist, ACMG Certified Guide, SAR Manager
Overall summary :
A dive into the reality of risk-managed mountain rescue, where the safety of the rescuer comes first, decisions are disciplined and shared, and technical skill becomes the linchpin of a successful mission.
Key issues :
- High call volume (>430 interventions/year), with a majority of non-medical assistance.
- Three core competencies structure our operations:
- Safe movement in complex alpine terrain.
- Essential medical care: airway management, immobilization, pain, recognition of signs of internal trauma.
- Technical rescue skills: evacuation, hoisting, avalanche risk management.
- Objective: reach subjects in less than 90 minutes in most zones.
Operating philosophy :
"Go home every night" - responder safety comes first.
Each mission is based on a two-dimensional risk assessment:
- Probability (reducing uncertainty by reading terrain, snow and wind conditions).
- Consequence (minimizing exposure and vulnerability: safer lines, ropes, avalanche transceivers, airbags).
Highlight - November 11 avalanche :
- Localisation : secteur de Spray Lakes Road ("Lone Ranger").
- Context: winds 45-60 km/h, 50-60 cm patches, difficult visibility.
- Critical decision: postpone intervention until the following day due to extreme danger.
- Day 2: controlled triggering by explosives (6 detonations, 6 major avalanches), then safe extraction.
- Lessons: decision-making discipline, importance of communication between guides, medical services and flight coordination.
Collaboration and medical care :
- Direct communication with paramedics and tertiary hospitals.
- Advanced discussion on the potential integration of ECMO in prolonged rescue (as in Europe).
Team culture and continuous learning :
- Every incident - including fatal accidents - is the subject of transparent feedback.
- Objective: to improve methods, strengthen cohesion and spread the safety culture throughout the alpine rescue community.
Key points:
- Risk management is based on preparation, discipline and the ability not to act when the danger outweighs the expected benefit.
- Professionalism is not measured by the number of interventions, but by the quality of collective judgment.

